

A vet-to-vet piece from South East Vet Referrals. Featuring Dr Richard Everson, RCVS Recognised Specialist in Veterinary Ophthalmology.
We see more ulcers than any other corneal problem, but many more never need us. An uncomplicated superficial ulcer may heal rapidly and that is the end of it. This piece is about three that don’t: the melting ulcer that progresses rapidly overnight, the superficial ulcer that stubbornly remains long after it was expected to have healed, and the cat with a brown/black plaque that no drop will shift. The common thread is timing. In each one, the eye that gets referred early has the best outcome.
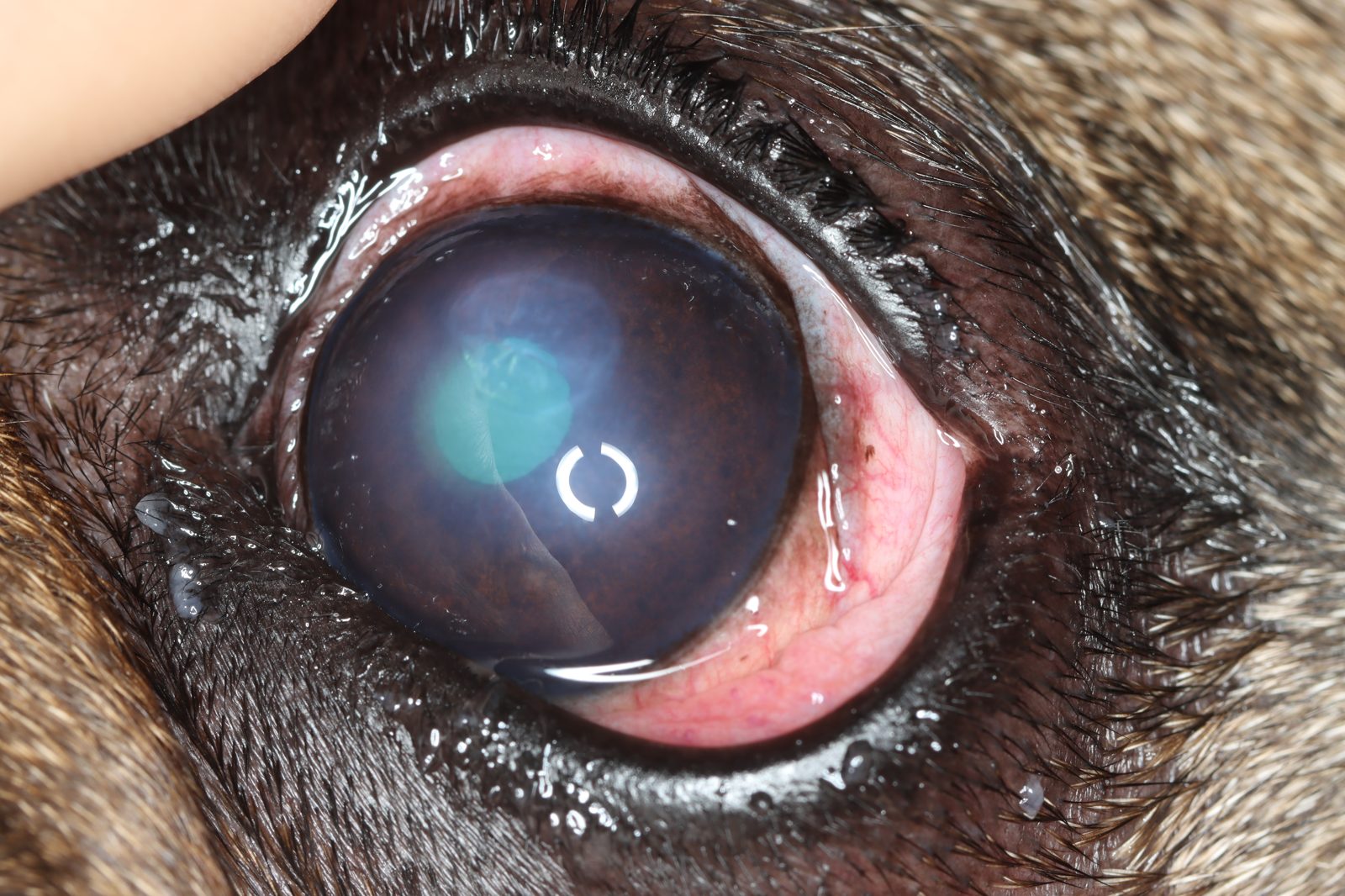
The brachycephalic eye that looks comfortable but isn’t
If there is one message worth holding onto from this piece, it is this: in a deep ulcer, apparent comfort is not reassurance. Examine for depth, not for pain.
Here is why. In a stromal ulcer, proteolytic enzymes (from invading bacteria, the patient’s own neutrophils, or from the cornea itself) digest the collagen matrix. The canine cornea is only around half a millimetre thick, and significant corneal thickness can be lost within hours in the worst melting ulcers. From the moment you recognise it, it is an emergency.

Brachycephalic breeds deteriorate faster, for stacked anatomical reasons grouped together as brachycephalic ocular syndrome: the lids may not fully cover the cornea when the patient is asleep, or with a normal blink, there is often medial entropion and trichiasis, the tear film is poorer, and the shallow orbit means the globe is more exposed. On top of all that, the brachycephalic cornea is less densely innervated and measurably less sensitive.
That last point is the dangerous one. Most of the corneal nerve endings are in the first third of the cornea, so as an ulcer deepens the blepharospasm and tearing you rely on as warning signs can fade just as the ulcer becomes most dangerous. A French Bulldog with a near-perforating descemetocele may sit holding the eye relatively open, creating the impression it is improving. Comfort, in these eyes, is not the all-clear.
What tells you a corneal ulcer is a surgical emergency
These are the findings that move a case from “treat and recheck” to “refer today”:
- Perforation: a positive Seidel test, a peaked or distorted pupil, a fibrin plug, or visible iris.
- A descemetocele: the stroma is gone down to Descemet’s membrane, leaving a crater whose clear floor does not take fluorescein while the rim around it stains. Perforation is close.
- Marked anterior uveitis driven by the cornea: aqueous flare, a miotic pupil, fibrin, or hypopyon.
- Any ulcer at roughly half stromal depth or more, and any melting cornea that is still enlarging despite aggressive medical treatment.
Medical therapy alone will not put tectonic strength back into a cornea that has lost this much tissue. That is the part a referral surgeon adds, and it is why these eyes need assessing sooner rather than after another recheck cycle.
While you arrange referral, the holding plan is a topical broad-spectrum antibiotic, an anti-collagenase such as autologous serum to slow the melt (given frequently), a topical cycloplegic to help manage the reflex uveitis, a systemic non-steroidal anti-inflammatory, and a buster collar.
The most useful adjustments for a brachycephalic patient are start serum sooner (perhaps even for a superficial ulcer) and to see back sooner. A 72 hour recheck that is perfectly safe in a mesocephalic dog can be too long in a brachycephalic one, think 24 to 48 hours.
The ulcer that won’t heal: think indolent, not infected
The second eye worth referring earlier is the superficial ulcer in a dog that simply won’t heal. If a superficial ulcer has not healed in the window you would expect, for example 5 to 7 days, think again about the cause.
An important cause of a ‘non-healing’ superficial ulcer in a middle-aged to older dog is a spontaneous chronic corneal epithelial defect (SCCED), the indolent or “Boxer” ulcer. The problem is not depth and not infection. New epithelium grows but cannot anchor to the stroma beneath it, due to the presence of a thick protein layer that shouldn’t be there. The giveaway on examination is a loose, redundant lip of epithelium at the margin, with fluorescein running underneath the edge as a faint halo. Antibiotic drops will not fix it.
A couple of things worth holding in mind. SCCEDs are very common in French Bulldogs, not just Boxers, but we can see them in any breed. They are more common in middle-aged to older patients. And it is a diagnosis of exclusion, so before you settle on it, rule out distichiasis, an ectopic cilium, entropion, a foreign body under the third eyelid, and dry eye (with a Schirmer tear test). A young dog is much less likely to have a SCCED, and any ulcer with stromal loss is not a SCCED (although it may have started as one!).
The fix is procedural rather than pharmacological: debriding the non-adherent epithelium and disrupting the abnormal protein layer so new epithelium can take hold. We most often use diamond burr debridement, which is well tolerated and effective, usually with a bandage contact lens too. The point for referral is simple: once an ulcer has failed to heal in the expected window, or failed a debridement or two, it earns another thorough assessment, rather than another fortnight of drops. That’s where referral comes in.
The cat with a brown plaque: corneal sequestrum
One condition that is rare in most species but common in cats is corneal sequestrum. This presents as an area of amber-to-black discolouration, often central, often with surrounding or overlying ulceration. It is an area of necrotic cornea and it is a condition that is not fully understood.

It is strongly breed-associated with Sphynx cats, Himalayans, Burmese, Persians and other flat-faced cats more commonly affected. We see sequestrum following corneal ulceration or irritation (caused by entropion, for example), and feline herpesvirus has been implicated. There is no medical cure. Topical treatment can settle the surrounding ulceration or a herpesvirus component, but it will not shift the sequestrum, and waiting for it to slough on its own is slow, unpredictable, and carries a perforation risk. The definitive answer is surgical removal under high magnification, usually followed by a graft to repair the cornea and reduce the risk of recurrence.
One genuine dog-and-cat divergence is worth flagging, because it catches people out: the grid keratotomy that helps an indolent ulcer in a dog should be avoided in cats, because this can trigger a sequestrum. So an amber or black corneal plaque in a cat is a sequestrum until proven otherwise, and a referral case rather than a medical one.
How do we repair a cornea with a deep ulcer or sequestrum?
The reason early referral pays off is that deep corneal disease is highly salvageable in the right setting. When too much stroma has been lost for medical therapy, or when sequestrum has been cut away, the surgeon rebuilds the structural strength of the cornea. Options include moving corneal tissue in a sliding flap (a corneo-conjunctival transposition), a conjunctival graft (bringing blood vessels to help halt malacia), donated cornea, and various biomaterials including amnion.
For a referring vet, the practical takeaway is that a deep or perforating ulcer is not a lost eye. It is an eye that needs to arrive with us urgently.
When to pick up the phone
If you are not sure whether a corneal case is one for us, call and talk it through. The shortcuts worth carrying into the consult room: in a flat-faced dog, trust the depth on examination over how comfortable the eye looks. In a middle-aged dog, a superficial ulcer without a clear cause, that has not healed in a week to ten days, may be a SCCED that needs intervention to heal. And in a cat, brown to black corneal discolouration is a sequestrum until proven otherwise. Refer any of those early, and the eye will thank you for it.