Medicine
Chronic Rhinitis
What is Chronic Rhinitis?
- Idiopathic lymphoplasmacytic rhinitis is the one of the most common forms of chronic nasal disease in dogs.
- Histopathology: Mixed inflammation, usually with lymphocytes and plasma cell predominating +/- eosinophils and neutrophils.
- Likely multifactorial: Aberrant immune response to inhaled antigens, secondary bacterial colonisation, and environmental triggers.
Differentials
- Neoplasia (30% cases in dogs and 40% in cats) – adenocarcinoma, lymphoma, neuroendocrine tumours
- Fungal rhinitis (Aspergillus spp.; cryptococcus)
- Foreign body
- Dental disease (tooth root abscess)
- Congenital defects (cleft palate)
- Polyps or anatomical abnormalities
- Systemic disease (hypertension, coagulopathies)
- NOTE – primary bacterial infection is extremely uncommon. Always look for an underlying aetiology
Clinical Signs
- Chronic mucoid-mucopurulent nasal discharge – usually bilateral (whilst unilateral disease is possible, this would be more common with focal lesions such as a foreign body or neoplasia)
- Sneezing +/- reverse sneezing
- Upper respiratory tract noise
- Lower respiratory signs can be due to concomitant lower respiratory disease or can be associated with post-nasal drip
- Facial asymmetry
Diagnostics
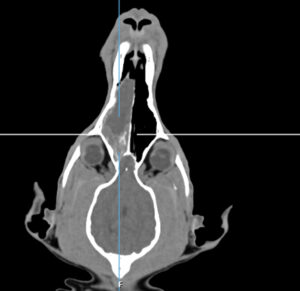
- Imaging:
- CT preferred vs radiography due to complex intranasal anatomy
- Rhinoscopy & Biopsy:
- Allows visualization of mucosa, mass lesions, fungal plaques
- Allows biopsies to be obtained from relevant lesions – lymphoplasmacytic inflammation vs neoplasia/fungal disease.
- Utility of biopsies is increased if targeted sampling performed.
- Microbial Assessment:
- Culture often unrewarding
- Additional Tests:
- Fungal serology, dental radiographs, bloodwork for systemic disease and coagulopathies.
Management
Goal: Symptom control and quality of life. Resolution of signs is very uncommon, and it is important to counsel the owner that this is commonly a lifelong condition with ongoing clinical signs.
Anti-inflammatory Therapy
- Anti-inflammatory therapy forms the mainstay of management; however, there is no definite consensus on the optimum medication or protocol to use.
- Cases tend to show variable responses with some responding favourably to NSAIDs and other to corticosteroids.
- Whilst oral steroids are often a good initial choice, ongoing inhalational therapy is often superior in terms of both efficacy and limitation of adverse effects.
Antibiotics
- Doxycycline: Used for its anti-inflammatory and immunomodulatory properties, even when bacterial infection is not confirmed. Pulse dose therapy is often advised.
Immunotherapy
- Allergen-specific immunotherapy: Beneficial if allergy testing identifies triggers.
- Other immunosuppressants:
- Cyclosporine: For severe/refractory cases or those who cannot tolerate steroid therapy.
Supportive Care
- Saline flushes, nebulisation, environmental control.
Surgical Intervention
- Reserved for neoplasia or severe anatomical obstruction.
Take Home messages
- Approximately one third of dogs with nasal signs have a sinonasal malignancy. This proportion is slightly higher in cats
- There are no reliable factors on clinical examination which confirm the underlying aetiology of nasal signs.
- Positive bacterial cultures are rarely useful or relevant. These are typically secondary to a primary underlying disease process with primary bacterial rhinitis being extremely rare.
- Early investigation with examination under anaesthesia, advanced imaging (CT vs MRI), rhinoscopy and biopsies should be advised to allow early diagnosis and superior outcomes especially given the relatively high proportion of neoplastic cases.
- Antibiotic therapy without a definitive diagnosis is contraindicated
- Blind nasal biopsies without appropriate imaging can lead to a high false negative results rate
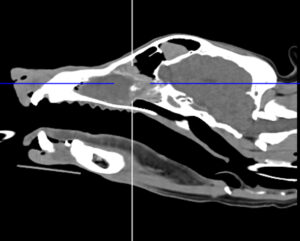
Nasal neuroendocrine tumour (diagnosed on rhinoscopic biopsy)

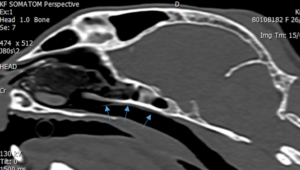
Grass blade in nasopharynx