
Neuro
IVDD
Intervertebral Disc Disease
Intervertebral Disc Disease (IVDD) is a common spinal condition in dogs that can cause symptoms ranging from back pain to paralysis. This document provides an overview of IVDD, including its anatomy, classification, clinical signs, diagnostic methods, and treatment options
Key points
- Acute intervertebral disc extrusion occurs in all breeds, more frequently in chondrodystrophoid dogs
- Plain radiographs do not provide adequate information
- MRI is the superior modality of investigations of spinal cord diseases
- The first 2 actions in all acute intervertebral disc diseases are
- 1. Restrict movement (cage rest)
- 2. Pain management (NOT steroids)
- Surgery should be considered for grades 4–5, and a history of progressive clinical signs
When to refer?

Detailed Information
Anatomy
The intervertebral disc has 3 main components
- annulus fibrosus (strong ring of collagen fibres)
- nucleus pulposus (cushion structure that adsorb shocks)
- endplates (in between the vertebrae)
The annulus and the endplates contain the nucleus pulposus in the middle of the intervertebral disc.
The nucleus pulposus is rich in collagen and proteoglycans, and the cells responsible for producing them are the notochordal cells (a remnant of the primordial structure in the early stages of the foetus). The collagen supports a scaffold for the proteoglycans, which have sulphate molecules that bind to water molecules. The nucleus is under a high-pressure environment and about 40 times smaller than it would be if not encased in the disc structure.
The annulus is a fibrous structure that keeps the vertebrae together, provides support to the spine, allows flexibility, and contains the nucleus pulposus. The collagen fibres are organised in multilayers that crisscross at each different level.
The endplate is a cartilage structure on each side of the vertebral body. The semipermeable endplate allows nutrition to cross to the nucleus pulposus and annulus. The intervertebral disc is the largest avascular structure in the body, and the function of the endplate is crucial in providing nutrition and oxygen.
Intervertebral disc degeneration or disease occurs when the collagen and proteoglycan degenerate. The reason for the degeneration is not completely clear. However, the gene for dwarfism is implicated, for example, in dachshunds. The notochordal cells disappear and are replaced by chondrocytes, the collagen changes structure, and the proteoglycans are broken down, with consequent loss of water molecules. This phenomenon is called dehydration, and the nucleus pulposus becomes stiffer. The degeneration in small breed dogs starts a few months after birth and is complete by the age of 12 months
During this process, there is a release of enzymes that tend to weaken the annulus fibrosus. The combination of stiffer nucleus pulposus and waken annulus fibrosus predisposes to intervertebral disc herniation. The Nucleus pulposus is ejected through the annulus and then impacts the spinal cord, causing a physical contusion. Depending on the speed of herniation, the clinical signs are different. The higher the speed, the worse the initial spinal cord injury. To aggravate the initial trauma to the spinal cord, the nucleus pulposus is now in an environment that can absorb more water molecules and swell up to 4 times its initial volume.
The disc herniation also triggers an inflammatory reaction, which can cause secondary irreversible damage to the spinal cord (myelomalacia). Whilst this is rare, it is devastating and there is no cure.
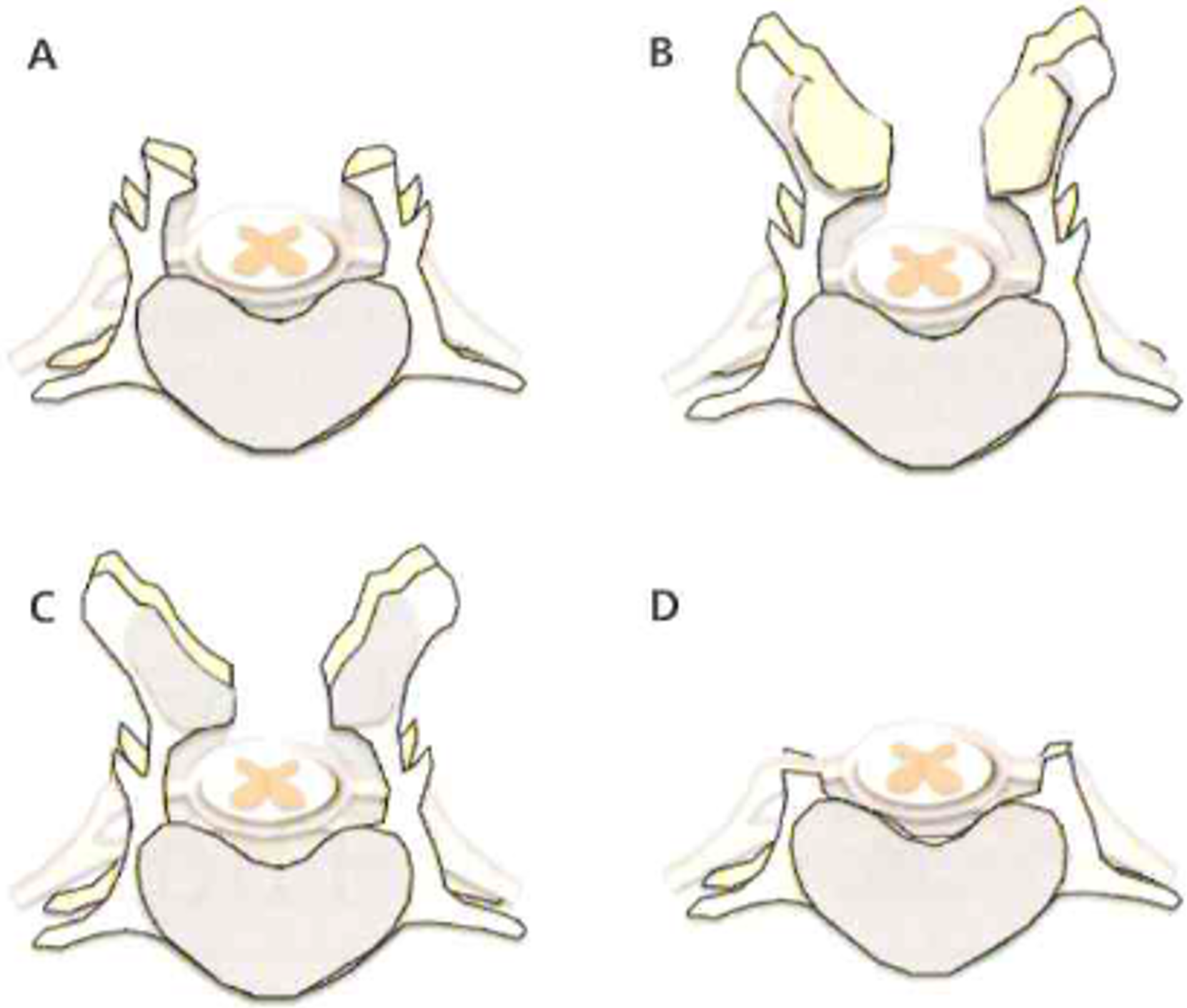
The current classification of IVDD include
- Acute non-compressive disc extrusion
- Acute hydrate intervertebral disc extrusion
- Intervertebral disc herniation Hansen Type 1
- Intervertebral disc herniation Hansen Type 2
- Acute Non-Compressive Disc Extrusion occurs without the previous degenerative process of the nucleus pulposus. A per-acute extrusion of a normal IVD nucleus is presumed to be associated with supra-physiological mechanical stress during athletic activity. A portion of the nucleus is explosively expelled through the annulus with great force, causing a focal contusive injury to the adjacent spinal cord, and its displacement can readily be observed on MRI. As the extradural material is nondegenerate and highly hydrated, it typically rapidly dissipates or is resorbed, leaving minimal to no spinal cord compression. This type of disk extrusion also sometimes has erroneously been referred to as “Fanquist type III” IVDD. Hansen used the term traumatic disc prolapse. These terms imply pre-existing disc degeneration, which is not commonly seen in this extrusion type. For these reasons, “acute non-compressive disc extrusion” has been adopted. The injury to the spinal cord associated with these explosive lesions varies widely but can be very severe (see below)
- Hydrate intervertebral disc extrusion is similar to acute non-compressive disc extrusion but distinctly different, in which material appearing hyperintense on T2W MRI scans is observed ventral to the spinal cord. These lesions have been described in the cervical region of dogs; the radiological interpretation, supported by surgical findings in some cases, is that the extruded material is hydrated nucleus pulposus and may be associated with moderate spinal cord compression; the severity of associated spinal cord injury is variable.
- Hansen Type I. Hansen described the pathological features of IVDD in dogs 60 years ago. Degeneration of the intervertebral disc leads to calcification of the nucleus pulposus and weakening of the annulus fibrosus. In time, the annulus fibrosus ruptures and releases the disc in the vertebral can, and spinal cord compression occurs. This extrusion can occur in any direction but is frequently dorsally directed because the nucleus is eccentrically positioned within the annulus. Hansen associated this type of degeneration with chondrodystrophic dogs and defined the subsequent nuclear herniation as “type I” IVDD.
- Hansen Type II. This type of herniation is also known as a bulging disc. Historically, this type of IVD degeneration was associated with non-chondrodystrophic dogs and can lead to disk herniation, defined as Hansen “type II.” More recent histologic analysis, although generally supportive of Hansen’s original descriptions, has suggested less difference between degeneration in chondrodystrophic and non-chondrodystrophic dogs than was previously assumed. Specifically, the more advanced stages of annulus fibrosus degeneration in non-chondrodystrophic dogs have shown the replacement of notochord‐like cells with chondrocyte‐like cells similar to the process in chondrodystrophic dogs. The annulus fibres become split from one another, allowing the accumulation of tissue fluid and plasma. With time and the mechanical pressure exerted by the nucleus (tending to be more dorsally directed), this degenerative process causes thickening of the annulus, especially dorsally. This can cause the annulus to protrude into the vertebral canal, which may compress the spinal cord or the spinal nerve roots.
Clinical signs
The clinical common denominators of intervertebral disc herniation are spinal pain and paresis or paralysis; importantly, these are not pathognomonic clinical features of IVDD. The onset and severity depend on the speed of herniation, the amount of nucleus pulpous herniated and associated damage to the adjacent vascular structures. Acute non-compressive disc extrusion, hydrate Intervertebral disc and Hansen Type 1 are generally peracute or acute and occur within seconds to hours. The catastrophic extrusion of the disc causes contusion to the spinal cord and damage to the spinal cord and vascular structure. The cascade of events following the contusion is responsible for further damage to the spinal cord, which can lead to myelomalacia (softening or liquefaction of the spinal cord). See separate information sheet.
Pain is often the first clinical sign seen in Hansen Type 1, likely due to the stretch and damage of the dorsal longitudinal ligament. This structure contains pain receptors sensitive to stretch. As the herniation progresses to affect the adjacent neural structures, meningeal and nerve root compression occur, causing further pain and neurological dysfunction.
The degree of spinal cord dysfunction is variable, and several classifications for thoracolumbar intervertebral disc herniation have been suggested. The most widely use is a grading from 0 to 5.
| Neurologic Grade | Clinical Signs |
|---|---|
| Grade I | Painful, with no neurologic deficits. |
| Grade II | Recurrent spinal pain with mild to moderate paraparesis (ambulatory, ataxic dogs). |
| Grade III | Severe paraparesis; non-ambulatory with pain. |
| Grade IV | Complete loss of motor function with intact sensory function; urinary incontinence and pain. |
| Grade V | Loss of all motor and sensory function; urinary incontinence with or without pain. |
This classification is helpful in formulating the prognosis, which varies with the severity of the clinical signs. In grades 1-3, the prognosis is generally favourable; in grade 4, it is fair and in grade 5, it is poor. Another poor prognostic factor is localisation. A lesion at the L4-S3 spinal cord segment is likely to damage the lower motor neurons and cause permanent neurological dysfunction.
Investigations
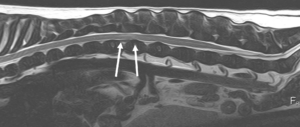
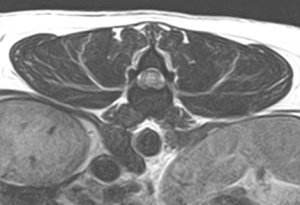
Magnetic resonance imaging (MRI) is the gold standard investigation for spinal cord diseases. Computed tomography, with or without myelography, is another modality that obtains diagnostic results similar to MRI. However, myelography increases the risk of complications. Radiography alone is not a suitable diagnostic modality in IVDD. In the past, myelography was commonly used to visualise the subarachnoid space; unfortunately, in the case of spinal cord swelling causing attenuation of the subarachnoid space, the interpretation could be difficult.
MRI is a superior method of investigation for the nervous system due to its ability to see the subarachnoid space, spinal cord, and soft tissue structure without using a contrast medium. The extruded disc material and its hydration can be easily identified. The image can be collected in several planes, adding confidence in the extruded material’s location and composition.
Radiographs can visualise calcified discs within the intervertebral disc space and, in some rare cases, within the vertebral canal. Calcified discs within the intervertebral disc space are not the cause of spinal cord dysfunction or pain.
Treatment
For all types of intervertebral disc herniation, the treatment protocols should include pain control, cage rest, anti-inflammatory drugs, careful nursing care for bladder management, comfort, hydration, and nutrition. The use of steroids should be avoided.
Non-surgical Management
This can applied in all cases presenting with a history compatible with intervertebral disc disease. The keyword for this approach is cage rest. The duration of the conservative management varies from 3 weeks to 6-9 weeks. In conjunction with cage rest, pain and bladder management are essential. The ideal candidate for this approach would be neurological grade I to III.
However, it is important to consider the history, particularly the progression. In our experience, dogs with progression of the clinical signs will require surgical management. Other scenarios of surgical management are persistent pain and unsatisfactory progression or improvements of the neurological dysfunction. The most common regime we recommend for conservative management is 3 weeks of cage rest; during this period, the dog would be allowed to go out 3-4 times daily for 10-15 minutes each time and physiotherapy when necessary. The owner should be monitoring the urinary function. In case of deterioration, they should contact us immediately. The deterioration of the clinical signs can occur at any point. On some occasions, these have occurred as soon as they left the hospital!
Pain management
Avoid steroids
Use NSAIDs if not contraindicated
Gabapentin/pregabalin in case of neuropathic pain
Use opioids when indicated
Paracetamol
Amantadine
Amitriptyline
In case of poor control of pain, surgical options should be considered.
Surgical spinal cord decompression has attracted some controversy. It has been observed that in some cases, the clinical signs improve in time without surgery. The current recommendation is to perform surgery in severe cases with a history of progression or lack of improvement with conservative management. Less severe cases can be managed conservatively with cage rest and NSAIDs. Spinal surgery should be considered if the clinical signs deteriorate or fail to improve, i.e., the dog is still in pain, ataxic, paretic, etc.
Type II intervertebral disc protrusion is generally slow and progressive, and surgery is often necessary.
Surgical management for intervertebral disc disease
Indicated when conservative management fails, the clinical grade is III to V, and the history indicates progression/deterioration of the neurological signs.
Standard surgical techniques
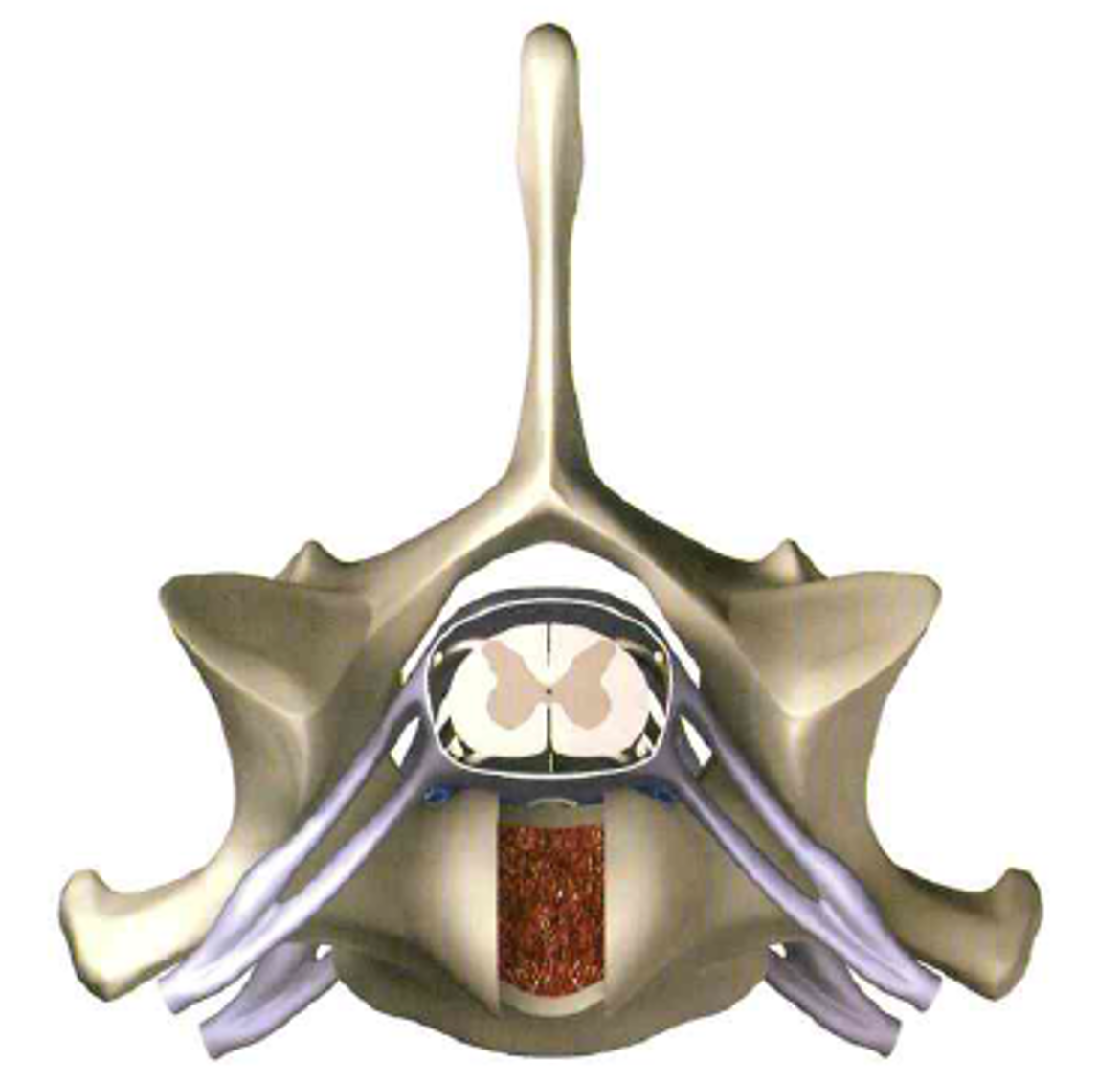
- Dorsal laminectomy
- Hemilaminectomy
- Mini-hemilaminectomy
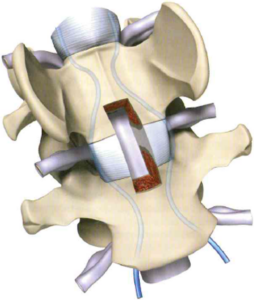
- Corpectomy
- Ventral slot
- Foraminotomy
- Laminotomy
- Fenestration
The techniques used in intervertebral disc disease depend on the anatomical area and location of the intervertebral disc (e.g., midline vs. lateralised discs), the size of the patient, and the presence of foraminal stenosis.
Hemilaminectomy is commonly used in thoracolumbar IVDD. The laminectomy involves the sacrifice of a vertebral articular process. It is also indicated in lateralised IVDD in the cervical spine and, in some cases, for neoplasia. The advantage of this technique is that the approach is relatively easy, and a good exposure of the spinal cord and the extruded disc can be obtained. The disadvantages are a predisposition to vertebral column instability, particularly in large breed dogs, and more significant risks to scar tissue adhesion, leading to laminectomy membrane formation. Later complications might be seen months to years after the surgery. The clinical signs associated with laminectomy membrane formation are pain and neurological signs.
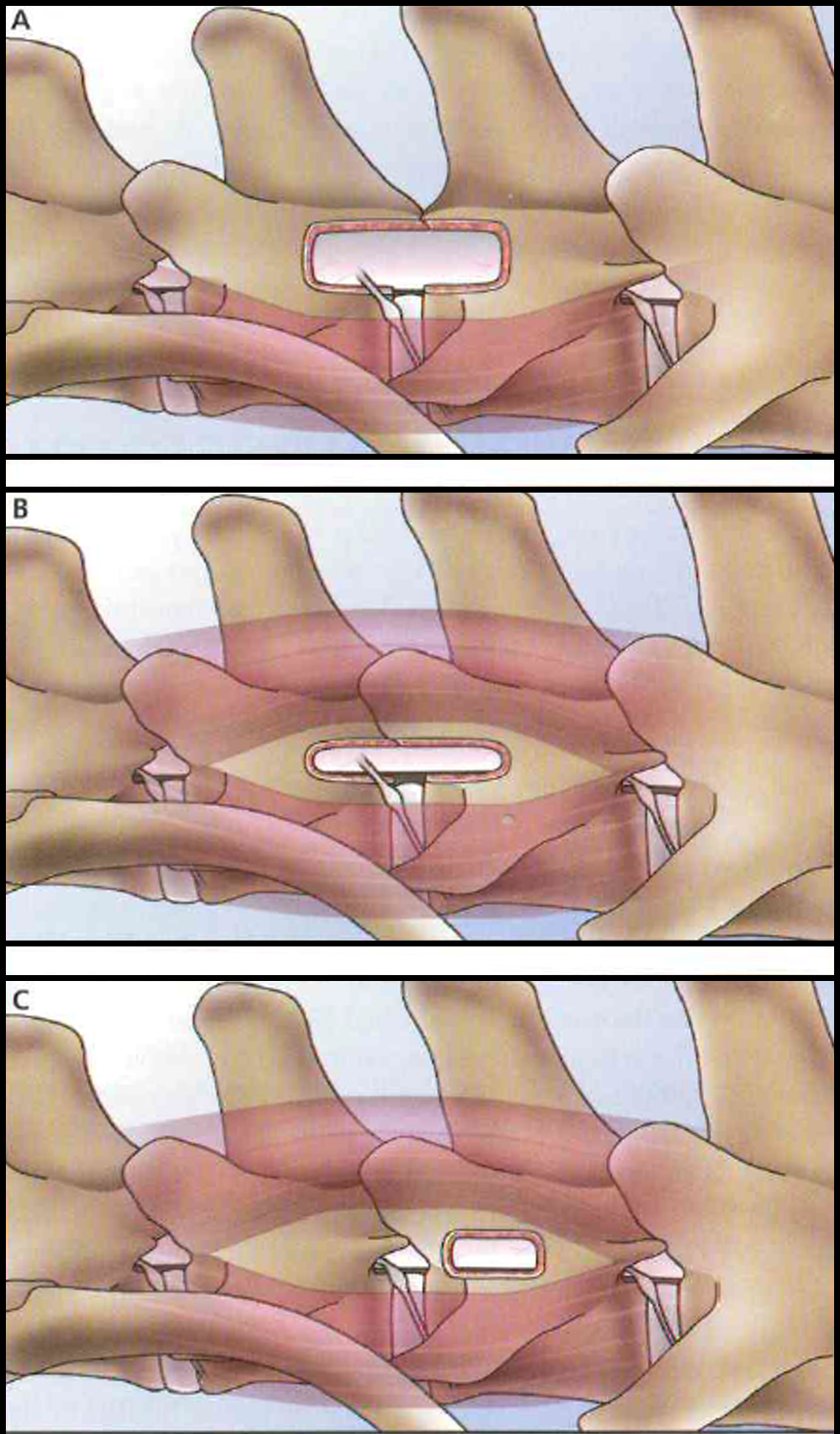
Mini-hemilaminectomy (pediculectomy/foraminotomy) requires more experience and good knowledge of the anatomy. The technique is mainly used in thoracolumbar IVDD, which is either acute or chronic. The advantage is the preservation of the articular process. If necessary, the technique can be extended to the vertebral body (corpectomy). This technique consists of removing a portion of the pedicle bone of 2 adjacent vertebrae to enlarge the intervertebral foramen essentially. It obtains excellent exposure to the nerve roots and dorsal annulus. It can sometimes be performed on both sides of the vertebra without causing instability. This is particularly useful in the case of bilateral chronic spinal cord and nerve root compression. Complications such as fractures of the articular facets and instability can occur if the laminectomy involves a large portion of the pedicles. This technique provides good exposure to the lateral-ventral spinal cord. It allows the retrieval of extruded disc material displaced ventrally or laterally with minimal spinal cord manipulation. Extruded material displaced dorsally might not be retrieved; however, the surgery can be easily converted into a hemilaminectomy.
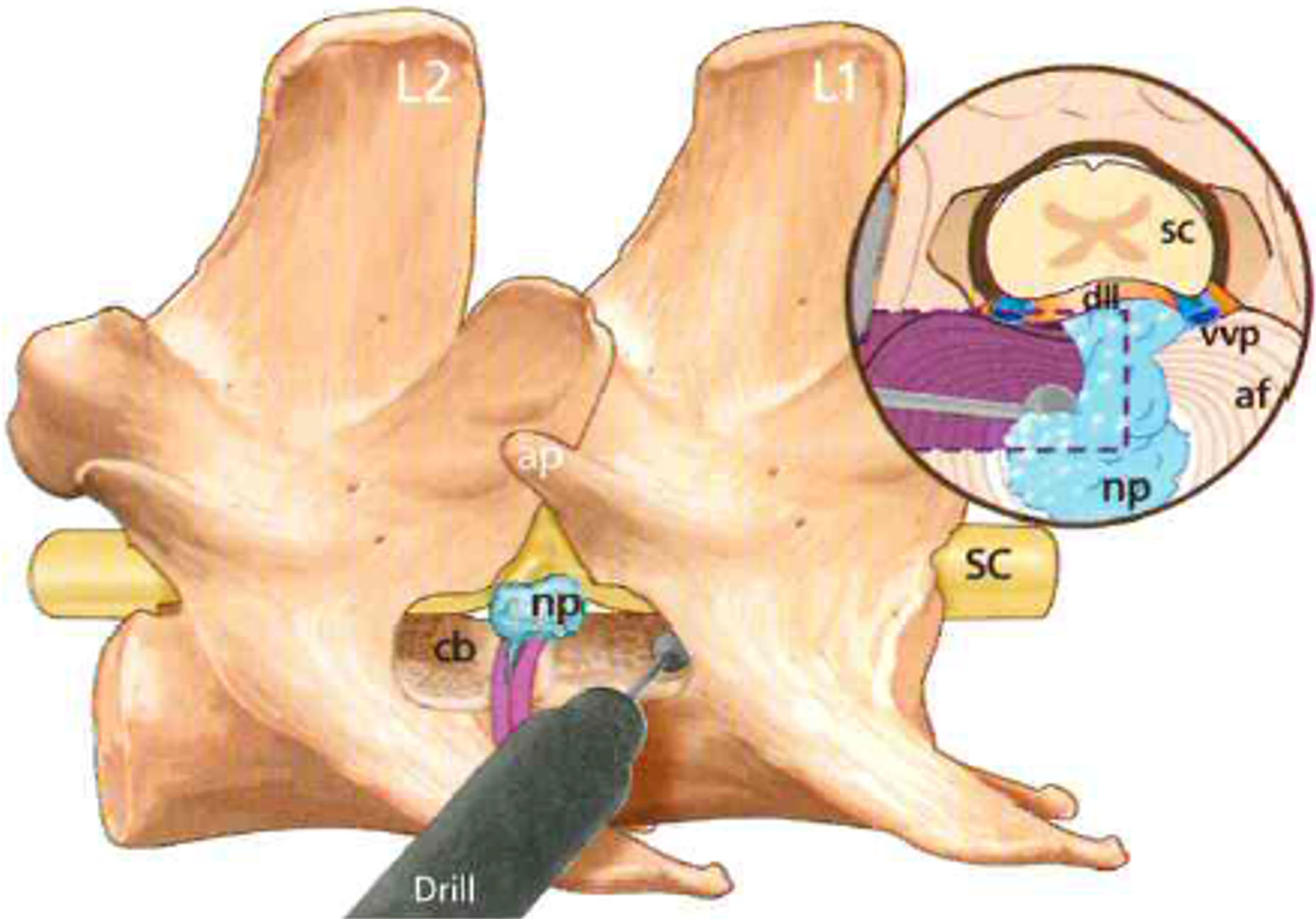
is indicated essentially for type II intervertebral disc disease. The protruding dorsal annulus is adequately exposed, and the spinal cord decompression is safely obtained with less manipulation of the spinal cord and decreased risks of incomplete removal of the annulus. The technique is challenging. The approach is ventrolateral, ventral to the paraspinal muscles and consists of partial removal of adjacent vertebral bodies that support the extruded/protruded disc material. The technique is helpful in large-breed dogs. The risks associated with this technique are nerve root damage, vertebral instability and sinus haemorrhage. However, the rate of complications reported is low. This is a relatively new technique (first reported in 1991) and an interesting alternative to dorsal approaches.
The ventral slot is used mainly in the cervical spine (neck). It is helpful for IVDD causing chronic or acute compression of the spinal cord. With this approach, mildly lateralised extrusion can be successfully treated. The advantages of this approach are the shorter surgical time, direct intervention on the IVDD, and minimal manipulation of the spinal cord. However, in large breed dogs, it can cause instability, and it is not suitable for cases of IVD instability or so-called wobbler syndrome. This technique can be combined with screws or pins and polymethylmethacrylate (PMMA) to obtain stabilisation in cases where instability is suspected or expected.
Pictures are from Rodolfo Cappello and some from the Book Current Techniques in Canine and Feline Neurosurgery; Andy Shores (Editor), Brigitte A. Brisson (Editor), ISBN: 978-1-118-43328-7, Oct 2017, which I co-authored a chapter.
Below is a summary of published surgical approaches and reported outcomes for canine acute intervertebral disc herniation (IVDH) affecting the thoracolumbar spine. Surgical approach Description Advantages Limitations Current Approaches to the Management of Acute Thoracolumbar Disc Extrusion in Dogs. Moore SA, Tipold A, Olby NJ, Stein V, Granger N; Canine Spinal Cord Injury Consortium (CANSORT SCI). Front Vet Sci. 2020;7:610. Published 2020 Sep 3. doi:10.3389/fvets.2020.00610
Dorsal laminectomy Removal of the spinous process and variable portion of the lamina with conservation of the articular processes
Advantages
- Increased cord exposure compared to hemilaminectomy
- Improved access to dorsal compressive lesions
Disadvantages
- No access to the ventral portion of the vertebral canal for disc removal
- Concern for laminectomy scar formation, particularly if more than one consecutive site
Hemilaminectomy Removal of half of the vertebral arch, including the lamina, pedicle, and articular process
Advantages
- Reduced laminectomy scar
- Improved access to the ventral portion of the spinal canal for disc removal
- Improved access for fenestration
Disadvantages
- Residual compression is common (clinical significance unclear)
Mini-hemilaminectomy/ pediculectomy is similar to a hemilaminectomy, but the articular process is spared.
Advantages
- Less invasive than hemilaminectomy
- Improved access to the ventral portion of the spinal canal for disc removal
- Improved access for fenestration
Disadvantages
- Residual compression is common (clinical significance unclear)
Partial corpectomy Partial removal of thoracic or lumbar adjacent vertebral bodies that support the extruded/protruded disk material inside the vertebral canal
Advantages
- Allows ventral decompression with minimal spinal cord manipulation
- It may offer an advantage for chronic and ventrally located disc herniations
Disadvantages
- Haemorrhage from the venous sinus is common
- Transient postoperative deterioration is common
- Residual compression is common (clinical significance unclear)
Fenestration without laminectomy Mechanical removal of the nucleus pulposus through a window created in the annulus fibrosus
Advantages
- Less invasive than laminectomy
- Good outcome for grade 1 and 2 injuries
Disadvantage
- Does not relieve spinal cord compression
- Reduced and prolonged recovery from severe injuries
Below is the outcome of dogs managed medically or surgically, based on the severity of presenting signs. Consensus statement on diagnosis and management of acute canine thoracolumbar intervertebral disc extrusion. Olby NJ, Moore SA, Brisson B, et al. ACVIM. J Vet Intern Med. 2022;36(5):1570-1596. doi:10.1111/jvim.16480
DPN, deep pain negative; DPP, deep pain positive; PP, paraparesis.
Spinal pain only and ambulatory PP
• Medical outcome 80% (115 dogs)
• Surgical outcome 98.5% (336 dogs).
• Comments: Lateral extrusion of disc material may lead to reduced response to medical management.
Non-ambulatory paraparesis
• Medical 81% (131 dogs)
• Surgical 93% (341 dogs).
• Comments: The level of recovery of non-ambulatory dogs was less complete with conservative management.
Paraplegia DPP
• Medical 60% (67 dogs)
• Surgical 93% (548 dogs).
• Comments: Recovery with medical management is prolonged and less complete compared to surgery
Paraplegia DPN
• Medical 21% (48 dogs)
• Surgical 61% (502 dogs)
Management post-surgery
Good analgesia is pivotal for a patient’s recovery. Pain control aims to reduce the physiological response to pain.
• Pain increases cortisol
• Upregulation of catecholamine release
• Upregulation of inflammatory mediators
• Cardiovascular changes
• Gastrointestinal complications
• Respiratory complications
Monitoring analgesia
The Modified Glasgow Composite Measure Pain Scale detects pain and its severity. If pain scores are greater than 4/5, analgesia is necessary.
Modified Glasgow Composite Pain Scale (mGCPS)
Vocalisation
[0] Quiet
[1] Whimpering or crying
[2] Groaning
[3] Screaming
Response to touch
[0] Do nothing
[1] Looks around
[2] Flinch
[3] Growl or guard area
[4] Snap
[5] Cry
Demeanor
[0] Happy and content and bouncy
[1] Quiet
[2] Indifferent or nonresponsive to surroundings
[3] Nervous, anxious or fearful
[4] Depressed or nonresponsive to stimulation
Posture/activity
[0] Comfortable
[1] Unsettled
[2] Restless
[3] Hunched or tense
[4] Rigid
Eating
[0] Eating normally
[1] Eating more slowly
[2] Eating with reluctance
[3] Not eating
Multimodal analgesia is recommended, and the combination of the following painkillers is effective in the first 24-48 hours from stabilising the patient, i.e. post-surgical
Opioids
• Methadone or
• Fentanyl CRI
• Ketamine
• Paracetamol
• Non-steroidal anti-inflammatory