

A vet-to-vet piece from South East Vet Referrals. Featuring Dr Richard Everson, RCVS Recognised Specialist in Veterinary Ophthalmology.
If there is one cataract message worth holding onto from this piece, it is this: the diabetic dog with developing cataracts should be referred early, not held back while you work to stabilise the diabetes.
It is an easy one to get the wrong way round, and completely understandable why. The instinct is to get the patient settled on its insulin first, then think about the eyes. But the lens does not wait for the bloods to behave. Diabetic cataracts can form remarkably fast, and a rapidly swelling lens can rupture. When that happens you are no longer looking at a planned procedure, you are looking at a sight-threatening emergency.
Why diabetic cataracts move so quickly

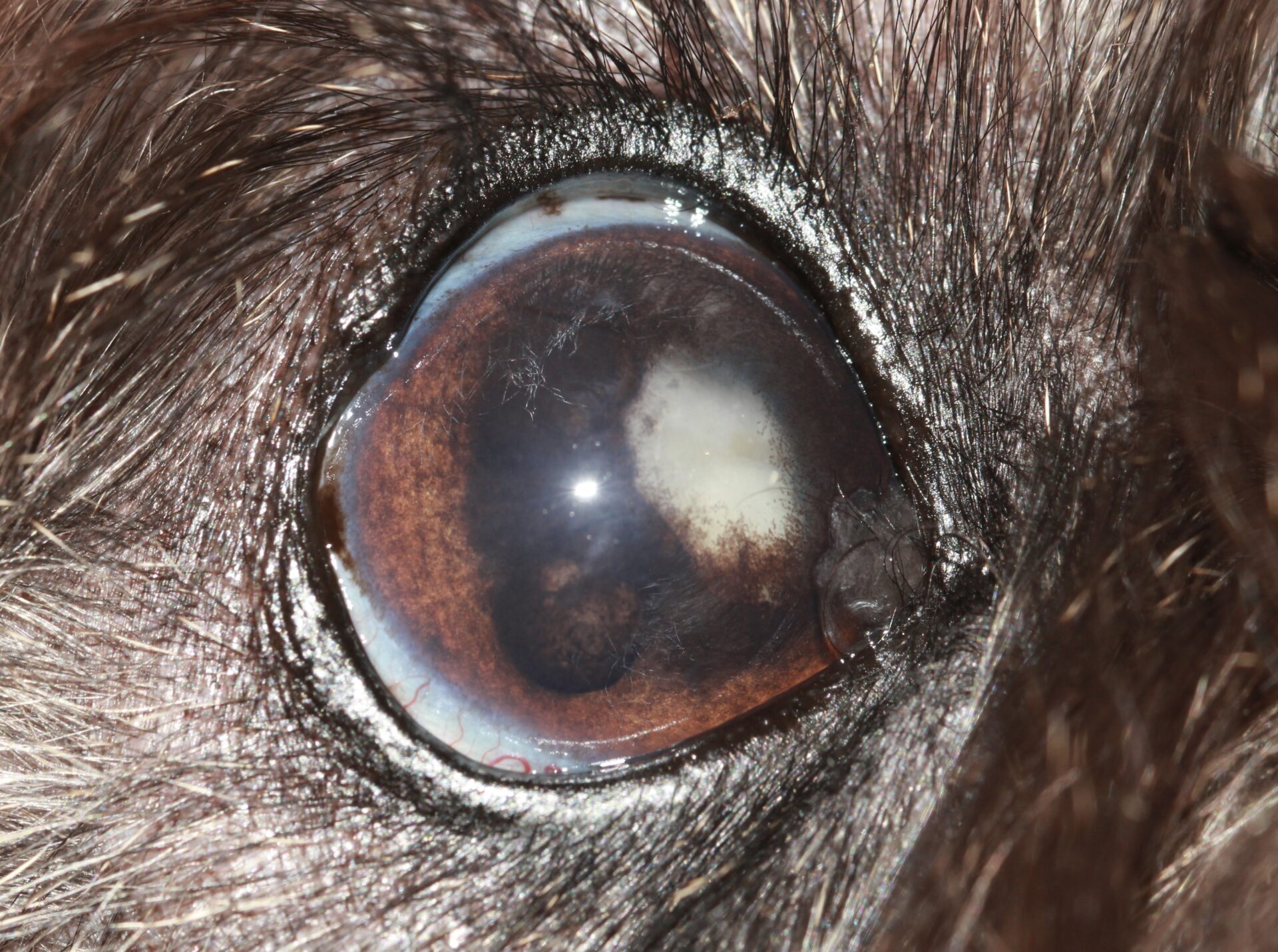
The canine lens is rich in an enzyme called aldose reductase. In a hyperglycaemic patient, the excess glucose entering the lens is converted to sorbitol, which cannot diffuse back out. Water is drawn in by osmosis, the lens fibres swell and the proteins are disrupted, and the lens goes cloudy. It is also why the problem is so much rarer in cats, whose lenses carry very little of the enzyme.
This mechanism is also why a diabetic dog can develop a cataract quickly. Around half of diabetic dogs develop cataracts within six months of diagnosis, and some progress a good deal faster than that. The practical consequence is that “let us get the diabetes stable and review in a few months” can quietly remove the dog’s best window for surgery. Stabilisation can take months; in that time the eye can progress to significant lens-induced uveitis, and in some cases to capsule rupture, secondary glaucoma or retinal detachment. At that point the dog may no longer be a surgical candidate at all.
The reassuring part: blood glucose does not need to be tightly controlled for us to operate. We would far rather see a diabetic dog early, with the diabetes still being worked on, than receive a well-controlled patient whose eyes have been left too long.
What this means in your consulting room this week
If you have a diabetic dog in front of you with cataracts, or suspected cataracts, three steps are worth taking before the patient leaves:
- Perform a Schirmer tear test. Dry eye is common in diabetics and easy to miss alongside the cataract.
- Start a topical non-steroidal anti-inflammatory to settle the lens-induced uveitis while referral is arranged. (Topical ophthalmic NSAIDs are human products used under the cascade; ketorolac and bromfenac are good choices.)
- Refer straight away. Do not park the eye pending diabetic stabilisation. Start the holding treatment and get the referral moving in the same consult.
The same “refer while it is still early” principle holds for non-diabetic cataracts too. Outcomes are better for an early cataract than for one that has been left for months or years, so if an owner would consider surgery, the time to assess is sooner rather than once the dog is blind.
Inside a cataract surgery, so you know what you are referring into
When you refer a cataract patient to us, here is the journey they go on, so you can set the owner’s expectations with confidence.
For a dog with cataracts in both eyes, we usually operate on both in the same visit. The patient comes in the afternoon before, and we ultrasound the eyes to check what is happening behind the cataract, because most of our patients have mature, white lenses we cannot see past. We take bloods and place an intravenous catheter, and the dog stays overnight.
Early the next morning we start the pre-operative drops to dilate the pupil and load it with anti-inflammatory, and the patient goes first on the list. Once under anaesthetic, we record an electroretinogram (ERG) to confirm the retina is still functioning, since we usually cannot see the fundus directly. Then we go to surgery. We make small corneal incisions, remove the cataract by phacoemulsification, and place an intraocular lens. In Richard’s hands a cataract takes around 30 to 40 minutes per eye; with prepping, positioning and draping, the patient is typically under anaesthetic for around two and a half hours.

The reason we like to operate early in the day is the recovery. An increase in pressure in the eye after cataract surgery is common, so we measure intraocular pressure every hour to begin with, which is far easier to do with a full day ahead of us. The patient stays a second night, by which point we are usually checking pressures every three to four hours and they are doing well, and goes home the following day.
After that, the rechecks step down gently: a week later, two weeks after that, then four to six weeks, three months, six months, and from then every six to twelve months. Dogs need more aftercare than people or cats here. Many of our canine patients stay on an anti-inflammatory drop long term to keep the eye comfortable.
The kit behind it
We operate with a current Bausch & Lomb phacoemulsification machine of the standard used in human cataract surgery, which makes lens removal possible and means our patients benefit from the most recent technology to make cataract surgery safer. We have a high quality Zeiss operating microscope with a built in video camera, so the nursing team and anaesthetist can follow each step of the operation in real time.
One case that stuck with us
Earlier this year we had a lovely dog booked in for cataract surgery who was, by reputation, extremely anxious around other dogs. Rather than hospitalise her overnight, with everything that entails, we adapted the whole pathway around her. The owner ran the pre-operative drop protocol at home. She came in through a side door for her ultrasound and left the same way. On the day of surgery she was kept in a separate part of the hospital, recovered, had her pressure checked, and went home the same night, then came back in the morning for her checks, in and out the side door each time.
She never met another dog across the entire course of her treatment, and she now walks in looking genuinely happy to be here. It is a small thing, but it is the kind of thing an independent referral setting can do: build the visit around the patient, not the other way around.
When to pick up the phone
If you are unsure whether a case is one for us, the easiest thing is to call and talk it through. For the diabetic dog specifically, the rule of thumb is the simplest one in this piece: if you suspect cataracts, start a topical NSAID, and refer early. The eye will thank you for it.